- Visibility 170 Views
- Downloads 29 Downloads
- DOI 10.18231/j.ijpi.2024.043
-
CrossMark

Management of Endo-Perio lesions by different modalities – A report of two cases
Introduction
The pulp-periodontal interrelationship is a unique one and may be considered as a single continuous system/one biologic unit interconnected with multiple pathways. This interrelationship influences each other during health, function and disease. When both systems are involved they are called true endo-perio lesions. Endodontic-periodontal problems are responsible for more than 50% of tooth mortality. An endo-perio lesion can have a varied pathogenesis which ranges from simple to extremely complex one. These lesions often present challenges to the clinician as far as diagnosis and prognosis of the involved teeth are concerned. It is very essential to make a correct diagnosis so that the appropriate treatment can be provided. To make a correct diagnosis the clinician should have a thorough understanding and scientific knowledge of these lesions and may need to perform restorative, endoontic or periodontal therapy, either singly or in combination to treat them.[1] This paper presents two such cases of endo-perio lesions managed by different modalities.
Case Report 1
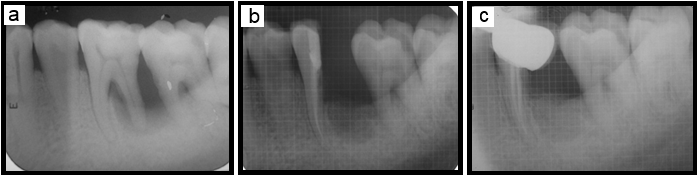
A 35 years old serving soldier reported with a chief complaint of pain and mobility in the lower left back tooth since last one month. On general physical examination, he was moderately built and nourished, well oriented to time, place and person. Intraoral soft tissue examination revealed a normal oral mucosa, except in relation to 36-37 region. The marginal gingiva in relation to these teeth showed moderate to severe gingival inflammation associated with probing pocket depth of 7 mm. Vitality testing of 36 revealed that the teeth were non-vital. IOPA radiographs wrt 36 showed vertical/angular bone loss pattern and circum radicular radioluscency wrt distal root of 36 giving an impression of primary periodontal lesion with secondary endodontic involvement.
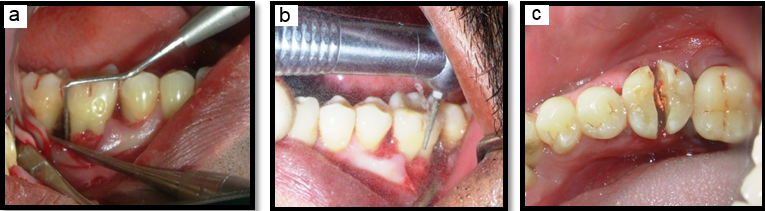
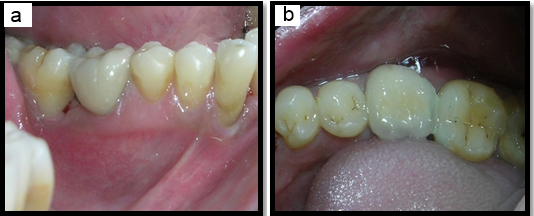
After obtaining an informed consent, the case was taken up for endodontic treatment 36 followed by surgical treatment 4 weeks after a thorough scaling, root planing and plaque control instructions. Intraoral disinfection was done with 0.2% chlorhexidine mouth rinse prior to administering local anesthesia with lignocaine HCl (1:200000). After adequate anaesthesia of the 35-37 region, incisions were made to reflect a mucoperiosteal flap. With the help of a long straight fissure bur, 36 was split exactly in the middle up to furcal area. ([Figure 1]) The distal root was removed, distal socket was curetted, irrigated and socket preservation was done using perioglass bone substitute. The mucoperiosteal flap was released apically allowing it to be positioned coronally without tension and achieve primary closure. ([Figure 2]) The periodontal dressing was placed over the surgical site and oral hygiene instructions were given. The patient was prescribed Tab Augmentin 625mg, Tab Combiflam thrice daily and instructed to rinse the mouth twice daily with 10 ml of 0.2% chlorhexidine mouth rinse for 5 days postoperatively. The case was reviewed after 02 weeks, the surgical site was irrigated with normal saline and sutures were removed, home care instructions were given. The healing of wound was satisfactory. The case was recalled after 04 & 12 weeks post operatively and has been taken up for prosthetic rehabilitation with resinbonded restoration at the end of 12 weeks.([Figure 3], [Figure 4])

Case Report 2
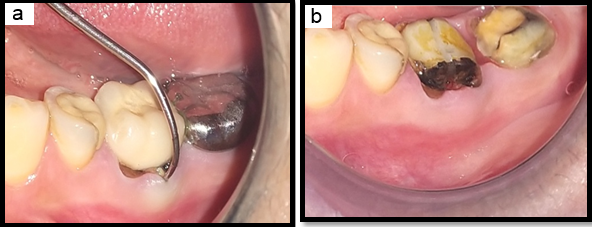
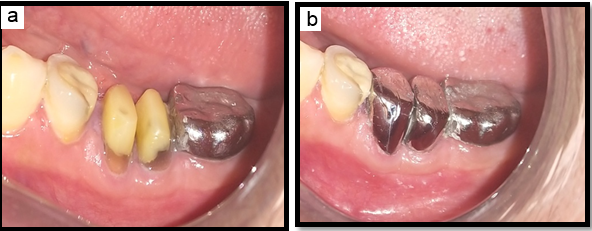
A 47 years old female patient reported with a chief complaint of pain in the lower left back tooth since last one week. On general physical examination, she was moderately built and nourished, well oriented to time, place and person. Intraoral soft tissue examination revealed a normal oral mucosa, except in relation to 36-37 region. The marginal gingiva in relation to these teeth showed moderate gingival inflammation. RVG image wrt 36 showed root canal treated 36 & 37 with full coverage crowns and radioluscency in the furcation area of 36, giving an impression of vertical fracture in the furcal area which could be correlated clinically. ([Figure 5], [Figure 6]) After obtaining an informed consent, the case was taken up for removal of metal crowns, followed by bicuspidisation & crown lengthening mesial and distal roots of 36 under local anaesthesia. The patient was prescribed Tab Augmentin 625mg, Tab Combiflam thrice daily and instructed to rinse the mouth twice daily with 10 ml of 0.2% chlorhexidine mouth rinse for 5 days postoperatively. The case was reviewed after 02 weeks, the surgical site was irrigated with normal saline and sutures were removed, home care instructions were given. The healing of wound was satisfactory. The case was recalled after 04 & 12 weeks post operatively and has been taken up for post & core of mesial and distal roots followed by prosthetic rehabilitation with two metal crowns, one each for mesial and distal roots at the end of 12 weeks. [2]
Discussion
The vast majority of pulpal and periodontal diseases are caused by bacterial infection. It has been suggested that cross-infection between the root canal and the periodontal ligament can occur via the anatomical (apical foramen, lateral and accessory canals, dentinal tubules and palato-gingival grooves) and non-physiological pathways (iatrogenic root canal perforations and vertical root fractures). [3] These pathways determine the spread of infection. Periodontal disease causes destruction of bone in a coronal-to-apical direction while direction of the endodontic lesions is from apex to coronal. When the pulp is infected, it elicits an inflammatory response of periodontal ligament. However, the effect of periodontal inflammation on the pulpal tissue remains controversial. [4] Clinically, the pulp is not affected by periodontal disease until accessory canals are exposed to the oral environment or microvasculature of the apical foramen is damaged. [5]
The endo-perio lesions present challenges to clinicians as far as diagnosis and prognosis of the involved teeth are concerned. The first step for proper diagnosis is the vitality tests. Although the vitality test cannot provide the histological status of the dental pulp, their ability to register pulp vitality is quite satisfied. The ability of vitality tests to detect non-sensitive reaction represented a necrotic pulp was reported as 89% with the cold test and 88% with the electrical test. [6] Proper endodontic treatment is a key factor for treatment success. Poor endodontic treatment allows canal re-infection and in this way, leads to the treatment failure.[2] Moreover, there are other contributing factors to cause endo-perio lesions. The tooth should be always evaluated in terms of any artificial pathways between periodontal and pulpal tissues such as cracks and fractures. The source of both infections should be removed.
If the rest of the dentition is periodontally healthy and any root cracks and fractures has been ruled out, healing of the periodontal tissues can be expected after endodontic treatment. Therefore, further treatment requirements should always considered followed by an observation period of at least 3 months. Conversely, there has been a debate in the literature about the impact of the endodontic treatment on the healing potential of the periodontium. Some studies have been reported that endodontic treatment may cause an inhibitory effect on periodontal wound healing,[7], [8] while some of them,[9], [10] have been demonstrated no significant effects. The prognosis of combined lesions mainly rests with the efficacy of periodontal therapy. [11]
The two modalities employed for the above cases are hemisection and bicuspidization. Hemisection refers to sectioning of the crown of a lower molar, with either the removal of one half of the crown and its supporting root structures, or the retention of both the halves, to be used after reshaping and splitting as two premolars. [12] The success of hemisection depends to a large extent on proper case selection. It is important to consider the following factors before deciding to undertake any of the separation procedures, advanced bone loss around one root with acceptable level of bone around the remaining roots, angulation and position of the tooth in the arch, divergence of the roots, length and curvature of roots and feasibility of endodontics and restorative dentistry in the root/roots to be retained. Contraindications for hemisection are calcified canals, root perforation in roots to be retained or fused roots making root separation almost impossible. Bisection/bicuspidization is the separation of mesial and distal roots of mandibular molars along with its crown portion.
The above procedures allow the root configurations to be changed sufficiently for a part of the root structure to be saved. However, the success of the hemisection/bicuspidisation procedures depends on the supporting bone, the restorative treatment plan, and the oral hygiene of the patient. The prognosis for hemisection is the same as for routine endodontic procedures provided due diligence is exercised in the case selection, the endodontic treatment has been performed adequately, the final restoration/prosthesis is of an acceptable design relative to the occlusal and periodontal needs of the tooth and patient’s compliance. Bicuspidization converts furcation-involved molars to single-rooted teeth and provide a favourable environment. Studies have reported that root resected molars had >90% survival rate, [13] whereas others reported about 30% of resected molars failed over a 10 year period. [14], [15] Furthermore, long term follow up is mandatory for these lesions.
Conclusion
A endo-perio lesion can have a varied pathogenesis which ranges from quite simple to relatively complex one. To make a correct diagnosis the clinician should have a thorough understanding and scientific knowledge of these lesions. Despite the segmentation of dentistry into the various areas of specialization, a clinician needs to perform restorative, endodontic or periodontal therapy, either singly or in combination. Therefore, to achieve the best outcome for these lesions, a multi-disciplinary approach should be involved.
Source of Funding
None.
Conflict of Interest
None.
References
- M Simring, M Goldberg. The pulpal pocket approach: Retrograde periodontitis. J Periodontol 1964. [Google Scholar]
- LB Peters, PR Wesselink, WR Moorer. The fate and the role of bacteria left in root dentinal tubules. Int Endod J 1995. [Google Scholar]
- M Zehnder, SI Gold, G Hasselgren. Pathologic interactions in pulpal and periodontal tissues. J Clin Periodontol 2002. [Google Scholar]
- S Seltzer, IB Bender, M Ziontz. The interrelationship of pulp and periodontal disease. Oral Surg Oral Med Oral Pathol 1963. [Google Scholar] [Crossref]
- WC Rubach, DF Mitchell. Periodontal disease, accessory canals & pulp pathosis. Periodontol 1965. [Google Scholar]
- K Petersson, C Söderström, M Kiani-Anaraki, G Lévy. Evaluation of the ability of thermal and electrical tests to register pulp vitality. Endod Dent Traumatol 1999. [Google Scholar]
- ML Morris. Healing of human periodontal tissues following surgical detachment and extirpation of vital pulps. J Periodontol 1960. [Google Scholar]
- JJ Sanders, WW Sepe, GM Bowers, RW Koch, JE Williams, JS Lekas. Clinical evaluation of freeze-dried bone allografts in periodontal osseous defects. Part III. Composite freeze-dried bone allografts with and without autogenous bone grafts. J Periodontol 1983. [Google Scholar]
- S Perlmutter, M Tagger, E Tagger, M Abram. Effect of the endodontic status of the tooth on experimental periodontal reattachment in baboons: a preliminary investigation. Oral Surg Oral Med Oral Pathol 1987. [Google Scholar]
- JLC de Miranda, CMM Santana, RB Santana. Influence of endodontic treatment in the post-surgical healing of human Class II furcation defects. J Periodontol 2013. [Google Scholar]
- I Rotstein, JH Simon. Diagnosis, prognosis and decision-making in the treatment of combined periodontal-endodontic lesions. Periodontol 2000. [Google Scholar] [Crossref]
- FS Weine. . Endodontic Therapy 1996. [Google Scholar]
- SY Park, SY Shin, SM Yang, SB Kye. Seung-Min Yang and Seung-Beorn Kye. Factors influencing the outcome of root-resection therapy in molars- A 10-year retrospective study. J Periodontol 2009. [Google Scholar]
- G Camevale, GD Febo, MP Tonelli, C Marin, M Fuzzi. A retrospective analysis of the periodontal-prosthetic treatment of molars withinterradicular lesions. Int J Periodontics Restorative Dent 1991. [Google Scholar]
- G Camevale, R Pontoriero, G Febo. Long-term effects of root-resective therapy in furcation-involved molars. A 10-year longitudinal study. J Clin Periodontol 1998. [Google Scholar]