Introduction
Breath malodor is a condition that has health and social implications. Halitosis is a complaint analogous to foul odor and describes any disagreeable odor in the breadth. Bad breath (oral malodor, halitosis) can be detrimental to one's self-image and confidence, causing social, emotional, and psychological anxiety.1
The importance of oral malodor goes beyond knowing its cause, diagnosis, and therapy because it interacts with other sociological issues such as culture, religion, race, sex, and social taboos.1, 2
Oral malodor is common and is of many types. Morning malodor is common, and it is probably due to increased microbial metabolic activity during sleep, which aggravates by a reduction in saliva flow during sleep. Malodor also caused by starvation, and it can be rectified easily by rinsing or cleaning the oral cavity with fresh water. Human lifestyles also influence malodor. This type of malodor is caused by the ingestion of certain foods and drinks or habits such as tobacco smoking and drinking alcohol.2, 3
The present review will focus on epidemiology, etiology and risk factors, diagnostic techniques, counseling aspects, and different treatment strategies in halitosis patients.
Epidemiology
Several studies in industrialized countries report a high incidence of moderate halitosis (> 50%), whereas severe cases are up to 5% of the total population. In most of the issues (> 85%), an etiological chain of breadth malodor originated from the volatile sulfur compounds (VSC), gingival and periodontal diseases.4
Large-scale studies showed that there is no gender predominance exists for breath malodor. The age distribution among halitosis patients can range from 5 to over 80 years. As gingival and periodontal diseases are the major causative factors for the incidence of breath malodor, the minor causative factors can also be identified, including ear-nose-throat pathology, metabolic disorders, renal disorders, respiratory and gastrointestinal pathologies.5 Halitophobia or imaginary breath odor, or pseudo halitosis is a particular category in which patients imagine halitosis. The patients persist in believing that he/ she has halitosis.
Etiology and risk factors
Humans emit various volatile and nonvolatile molecules that are influenced by genetics, diet, stress, and disease. Intraoral and extraoral causes originate halitosis. In more than 85% of cases, halitosis is originated from the oral cavity, mainly from a complex interaction between the Gram-negative anaerobic microorganisms.5, 6
Medical risks for bad breath include: Bronchial and lung infections, Chronic sinusitis, post-nasal drip, tonsillitis, cold or flu, untreated nasal polyps, diabetes, syphilis, diseases of the stomach and lungs, liver, kidneys, gallbladder dysfunction, various carcinomas, and some medications can cause or exacerbate bad breath.6, 7
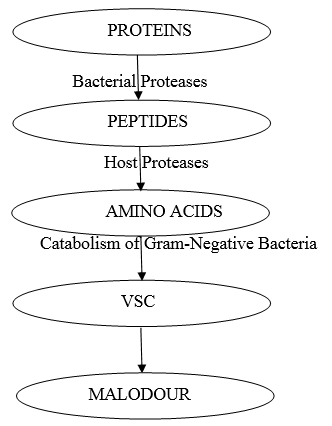
Bacteria play an essential role in the production of malodor. According to McNamara et al., malodor components were formed from incubated saliva with a shift in Gram-positive microorganisms to Gram-negative anaerobic microorganisms. The following are the putative malodorous species identified. They are mainly Gram-negative anaerobic microorganisms that depend primarily on proteins, peptides, or amino acids and degrade them into volatile sulfur compounds (VSC).7, 8
Volatile Sulphur Compounds
Volatile sulfur compounds are the gases that have demonstrated a higher correlation with halitosis. Volatile aromatic compounds (indole and skatole) and amines (cadaverine) also contribute to malodor.9
Volatile sulfur compounds are mainly produced through putrefactive activities of bacteria present in saliva, the gingival crevice, the tongue surface, and other areas. Production and release of the VSCs appear to depend on many local factors. For example, Bacterial population: predominance of gram-negative anaerobes and Physical-chemical conditions: salivary pH and oxygen depletion. The following tables explain the different VSCs and their production.9, 10
Table 1
Prevalence studies concerning Halitosis
Table 2
Microorganisms
|
• |
Microorganisms |
|
• |
Selenomonas |
|
• |
Peptostreptococcus |
|
• |
Eubacterium |
|
• |
Centipede |
|
• |
Bacteroides |
|
• |
Fusobacterium |
|
• |
Porphyromonas gingivalis |
|
• |
Porphyromonas endodontalis |
|
• |
Treponema denticola |
Table 3
Volatile Sulfur Compounds
Table 4
The following are the main methods to diagnose oral malodor:
Table 5
Classification of malodor with corresponding treatment needs
Diagnosis
Dental professional consider bad breath seriously, whether they appear justified or not. Before diagnosing bad breath, clinicians must still rely on their noses to distinguish the main types of oral odors. These include (i) periodontal-type odor which usually comes from periodontal pockets and interdental spaces; (ii) odor from the posterior tongue dorsum (iii) denture odor, (iv) characteristic nasal odor, and (v) smoker's halitosis. All these odors become distinct and recognizable, with practice and experience, even when found in various combinations.10, 11
Instructions to the patient and examiner before halitosis test
Patients are instructed to avoid taking antibiotics before three weeks of the test. It is essential to teach patients not to eat foods containing garlic, onion, and spices at least two days before the halitosis assessment. Avoiding alcohol consumption, smoking, brushing and eating food at least 12 hours before the assessment time.
During screening, the clinician should have a normal sense of smell, and he should avoid any cosmetics before the assessment. For a better diagnosis, it is essential to do the test at several appointments on different days.12
Counselling Aspects
The causation of bad breath is multi-factorial and may involve both oral and non-oral sources.
Even the medications, especially those that reduce salivary flow, may contribute to offensive breath odor.12, 13
Even after the elimination of offensive foods and beverages, some patients need the dentist's expertise. As there is advanced information regarding diagnosing and managing malodor, it is important that the dental professional shouid feel comfortable sharing this information and these products with their patients.14
Experienced, confidant dental health professional is considered the most reliable method of confirming a chronic breath odor problem.
Dental health professionals need to be comfortable with explaining the etiology of and treatments for oral malodor to their patients witout any hesitation.
Dentists should be familiar with the interviewing and counseling techniques that encourage open communication, reduce anxiety, and establish rapport.15
Clinical Management
One of the best method to manage bad breath is to instill patients with good oral hygiene practices and ensure that their dentition is maintained correctly.
Tongue scraping should be an essential daily routine along with brushing the teeth. A variety of tongue scrapers has been produced in recent years. tongue scraping or cleaning can also be performed by toothbrush that minimizes the gagging reflex. Tongue odor, can be reduced by brushing the tongue in a gentle but thorough manner.16
Bad breath is severe when the mouth dries out at night, while fasting). Maintaining water balance throuh out the day helps in managing bad odor. Chewing gum is also an alternative to reduce bad breath during the day. However, its use should be restricted to only a few minutes at a time to avoid temporomandibular joint problems.17
In patients with malodor of oral origin, even after carrying out best oral hygiene practices, rinsing and gargling with any efficacious mouthwash may be a right choice. However, it is well known that many types of mouthwash contain components that may have a non-beneficial effect on oral tissues. The right time to use a mouthwash is probably before bedtime, because (i) remnants of the mouthwash that remain in the mouth for a longer period have an extreme effect; and (ii) bacterial activity is also greatest during the nighttime when saliva flow is practically zero, and microbial activity is highest.14, 17
The patients will feel difficult to sense the reduction in halitosis immediately after consulting the dental profession. This can be best addressed with the help of the "confidant," who can monitor changes over time. In those cases in which the odor persists even after the treatment strategies patient should be referred back to the physician for further assessment.14, 16, 17
Conclusions
In recent times, however, there is a growing awareness that bad breath is a problem which the dental professions should identify and address. Together with the increasing interest of dental professionals in bad breath diagnosis and treatment, there has been an adjacent increase in research activity in this field,
The central concepts in diagnosis and treatment of oral malodor are:
Bad breath is a common condition that usually comes from the mouth itself and rarely from the gastrointestinal tract. The posterior dorsum of the tongue is the most frequently overlooked source of bad breath.
The dentist is s the first person who identifies and diagnoses the lousy breath
Appointment for the patients complaining of bad breath should be assigned a separately and encouraged to come with the family member or close friend (confidant).
Although many quantitative measurement techniques are available and helpful, the clinician should also make a differential judgment based on the actual smelling of the odor emanating from the patient's mouth and nose.
Bad breath can be facilitated by proper dental care, oral hygiene, deep tongue cleaning, and, if necessary, rinsing with an effective mouthwash.
If the problem persists, the patient should be promptly referred for appropriate medical care